



No Air Up There
Hypoxia Awareness
By Jennifer Caron, FAA Safety Briefing Magazine Copy Editor
Mid-flight is not the time to learn about hypoxia, the medical term for oxygen deficiency. It doesn’t give you much warning, and if you don’t detect it early enough, it can be a real killer. Some pilots believe that living at a higher altitude offers significant protection from hypoxia. This is partially true. Without question, someone who lives at 9,000 feet will handle an excursion to 12,000 feet better than someone who lives at sea level. However, this benefit can rapidly decrease and is subject to individual variability.
Hypoxia is an inherent risk for many in aviation, but there are regulatory requirements and training designed to mitigate it.
The Rules and the Regs
For the general aviation pilot, 14 CFR section 91.211 applies. While most of us are familiar with the need for oxygen above a cabin pressure altitude of 12,500 feet mean sea level (MSL) for flights over 30 minutes and all flights above 14,000 feet MSL, keep in mind there are additional rules for pressurized aircraft in paragraph (b).
Dr. Susan Northrup, FAA Federal Air Surgeon notes that many FAA resources and training tools cover hypoxia, including:
- Advisory Circular (AC) 61–107B CHG 1, Aircraft Operations at Altitudes Above 25,000 Feet Mean Sea Level or Mach Numbers Greater than .75.
- FAA’s Pilot Handbook of Aeronautical Knowledge, Chapter 17.
- Videos (e.g., be/E56AmOTSues), Aeromedical Safety Brochures, and an in-person, one-day course in Oklahoma City. The latter includes training in either the altitude chamber or the PROTE (Portable Reduced Oxygen Training Enclosure).
Symptoms
Everyone’s response to hypoxia varies. Unless you’ve had special training to recognize its symptoms, hypoxia doesn’t give you much warning. It steals up on you, giving your body subtle clues.
The order of symptoms varies among individuals and include the following:
- Increased breathing rate
- Headaches
- Lightheadedness
- Dizziness, tingling, or warm sensations
- Sweating
- Poor coordination, impaired judgment, tunnel vision, and euphoria.
See FAA’s Aerospace Medical Education Division’s (AMED) online hypoxia brochure to learn more about how to recognize your symptoms of hypoxia.
PROTE-able Training
To recognize the onset of hypoxia, you can do so safely, and on the ground in altitude training devices that allow participants to breathe air with a lower percentage of oxygen. A quick internet search will show a number of commercial providers who offer this training.
The FAA version of this training is the Portable Reduced Oxygen Training Enclosure, or PROTE, a traveling altitude training device.
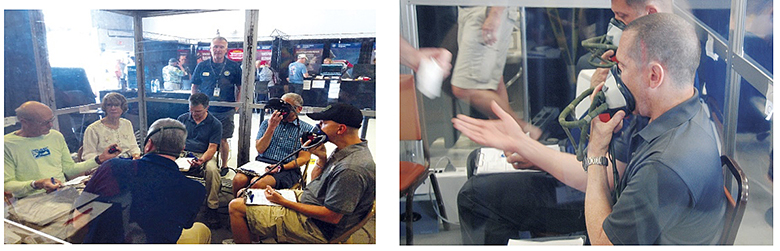
Photo of participants in the FAA’s PROTE system.
Besides the physiological training course with altitude chamber and vertigo demonstrations, you can also take a one-day survival course at FAA’s Civil Aerospace Medical Institute (CAMI) in Oklahoma City.
O₂ Equipment
A basic knowledge of oxygen equipment can be critical whether you are flying a commercial, commuter, or a general aviation aircraft. This equipment is the first line of defense against the potentially lethal effects of hypoxia and carbon monoxide poisoning. It is the responsibility of the pilot that all aboard the aircraft — crewmembers and passengers — know how to use this life-saving equipment safely and efficiently.
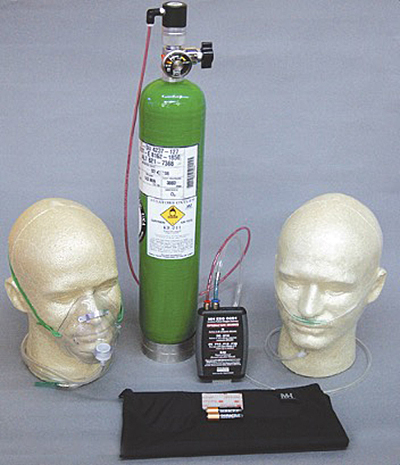
Photo of oxygen equipment.
Per FAA’s brochure on oxygen equipment use in GA, there are three components to most oxygen systems, whether they are portable or installed systems.
- A storage system (containers)
- A delivery system
- Mask or nasal cannula
Storage Systems
Oxygen can be stored in the aircraft as a gas, liquid, or a solid.
As a gas, the gaseous aviator’s breathing oxygen (ABO) has the major advantage of being more economical. It can be stored in high-pressure (1800–2200 psi) containers or low-pressure (400–450 psi) containers. The major disadvantage is the weight and bulk of the storage containers, which may become an issue in smaller aircraft.
As a liquid, oxygen can be serviced to the aircraft in a liquid state, the liquid aviators breathing oxygen (LOX). The advantage of LOX is that it has a nine hundred-to-one expansion ratio. In other words, one liter of LOX will expand into 900 gaseous liters of ABO. This provides a three-to-one space and a five-to-one weight savings over gaseous ABO. The major disadvantages are that LOX is stored at its critical temperature of minus 197º F and its volatile nature when it comes in contact with petroleum products. If LOX comes in contact with exposed skin, severe frostbite may occur.
As a solid, sodium chlorate candles (solid-state oxygen candles) have the advantage of saving weight and space over ABO because they provide a six hundred-to-one expansion ratio. The major disadvantage is that once the chemical reaction starts (the candle is activated), it can’t be stopped easily. Additionally, the candle produces a great deal of heat and precautions must be taken to avoid a fire hazard. Improper shipping of unexpended oxygen candles was the cause of the ValuJet crash from the mid 90’s. So this is a major possible safety issue.
There are also molecular sieve oxygen generators (MSOG) that take ambient air and separate oxygen from the nitrogen and inert gases. The separated oxygen is concentrated and used to supply the aircraft. The military has used this system for many years, as well as medical patients who need a portable oxygen system. Civil aviation hasn’t embraced MSOG, but it may become more common in future aircraft.

The results of a servicing error where high pressure oxygen was used to fill a low pressure system.
Delivery Systems
Oxygen delivery systems deliver oxygen from the storage containers.
Typically used at 28,000 feet and lower, continuous flow is economical in that it doesn’t need complicated masks or regulators to function, but it is also very wasteful — the oxygen flow is constant whether you’re inhaling, exhaling, or pausing in between breaths.
The diluter demand system, typically used at altitudes up to 40,000 feet, compensates for waste by giving the user oxygen on-demand (during inhalation) and stops the flow when the demand ceases (during exhalation).
Pressure demand systems provide oxygen under positive pressure that slightly over-inflates the lungs allowing you to fly at altitudes above 40,000 feet, where 100% oxygen without positive pressure is insufficient.
Masks and Nasal Cannulas
Oxygen masks and cannulas need to be compatible with the delivery system you are using.
Quick-don masks must have the capability to be donned with one hand in five seconds or less, while accommodating prescription glasses. Typically rated to altitudes up to 40,000 feet, these masks are usually suspended or stored to permit quick and unimpeded access by flight deck crew.
Airline drop-down units (“Dixie cups”) look similar to a GA re-breather mask. However, they function differently and allow users to go to higher altitudes. Used at altitudes up to 40,000 feet, Dixie cups use an external reservoir bag and a series of one-way valves working in sequence to allow a mixture of 100% oxygen and cabin air into the mask. Activated by pulling down on a suspended mask, oxygen from a supply source flows continuously into the reservoir bag.
During inhalation, a one-way valve allows the flow of oxygen from the reservoir bag into the lungs. If the reservoir bag empties before inhalation is complete, a second one-way valve on the mask face piece opens to permit the flow of cabin air into the mask, allowing the user to take a full breath. If the user is breathing rapidly, the reservoir bag will appear to not fully inflate. Expired air is vented out of the mask into the cabin via a one-way exhalation valve; expired air is not returned to the reservoir bag.
Know the equipment you have on board, know when to use it, and most importantly, know its limitations. It’s your key to a safe and enjoyable flight.
Nasal cannulas are continuous-flow devices and offer the advantage of personal comfort. They are restricted by federal aviation regulations to 18,000 feet service altitude because of the risk of reducing blood oxygen saturation levels if one breathes through the mouth or talks too much.
Oral-nasal re-breathers are the most common, the least expensive, and the simplest to use. Supplying adequate oxygen to keep the user physiologically safe up to 25,000 feet, rebreathers have an external plastic rebreather bag that inflates every time you exhale. The purpose of the rebreather bag is to store exhaled air so that it may be mixed with 100% oxygen from the system.

An example of a nasal cannula system.
For a more detailed overview of aviation oxygen system installations in non-pressurized aircraft, see chapter six of AC 43.13–2B, Acceptable Methods, Techniques, and Practices for Aircraft Alterations.
Check It
With any system you use, and prior to every flight, you should perform the “PRICE” check to inspect oxygen equipment.
PRICE CHECK PLEASE!
PRESSURE: Ensure that there is enough oxygen pressure and quantity to complete the flight.
REGULATOR: Inspect the oxygen regulator for proper function. If you are using a continuous-flow system, ensure that the outlet assembly and plug-in coupling are compatible.
INDICATOR: Don the mask and check the flow indicator to ensure a steady flow of oxygen.
CONNECTIONS: Ensure that all connections are secured. This includes oxygen lines, plug-in coupling, and the mask.
EMERGENCY: Keep oxygen equipment in your aircraft ready to use for emergencies that require oxygen (e.g., hypoxia, smoke and fumes, rapid decompressions/decompression sickness). Also, brief passengers on the location of oxygen and how to use it.
Know the equipment you have on board, know when to use it, and most importantly, know its limitations. You can learn more about the O₂ equipment you need for a safe and enjoyable flight by downloading FAA’s brochure (PDF).
Jennifer Caron is FAA Safety Briefing’s copy editor and quality assurance lead. She is a certified technical writer-editor in the FAA’s Flight Standards Service.
Reprinted with permission from FAA Safety Briefing. Visit the Flight Safety Briefing website: https://www.faa.gov/news/safety_briefing/